

The Billing System Was Never Built to Handle This Much Complexity
Healthcare billing is broken. Not slightly off — structurally, fundamentally broken in ways that have compounded quietly for decades.
Talk to any RCM director who’s been in this industry longer than ten years and they’ll tell you the same thing: the workflows haven’t changed, but everything around them has gotten dramatically harder. More payer rules. More code specificity. More prior auth. More denials. And somehow, the expectation is that the same lean billing teams — often understaffed, consistently under-resourced — will absorb all of it without missing a beat.
They can’t. And the numbers in 2026 make that impossible to ignore.
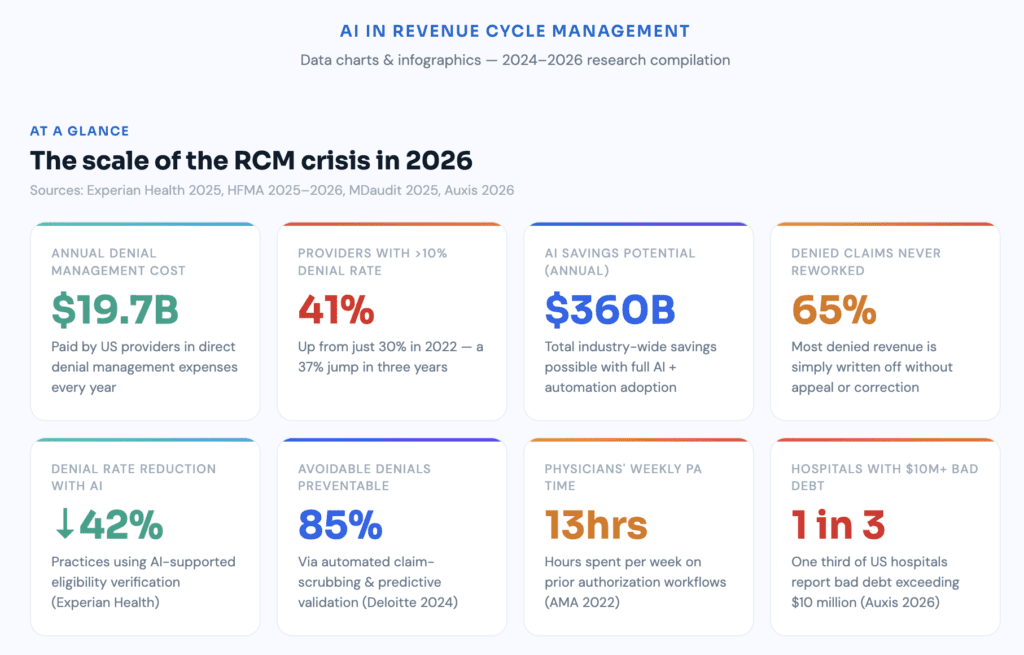
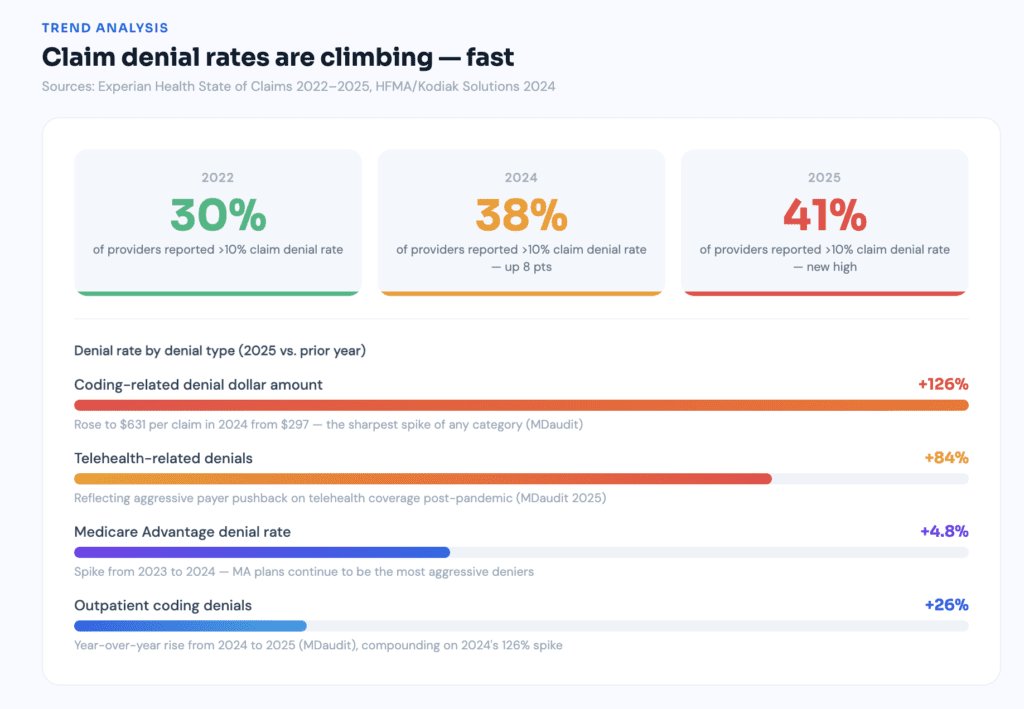
Initial claim denials hit 11.8% in 2024, up from 10.2% just a few years earlier. The trajectory since then has only gotten steeper. In 2022, 30% of providers reported that at least 10% of their claims were denied. By 2024, that figure had grown to 38%. In 2025, 41% of providers reported denial rates exceeding 10%. That’s not a trend. That’s a slow-motion financial crisis, and it’s accelerating.
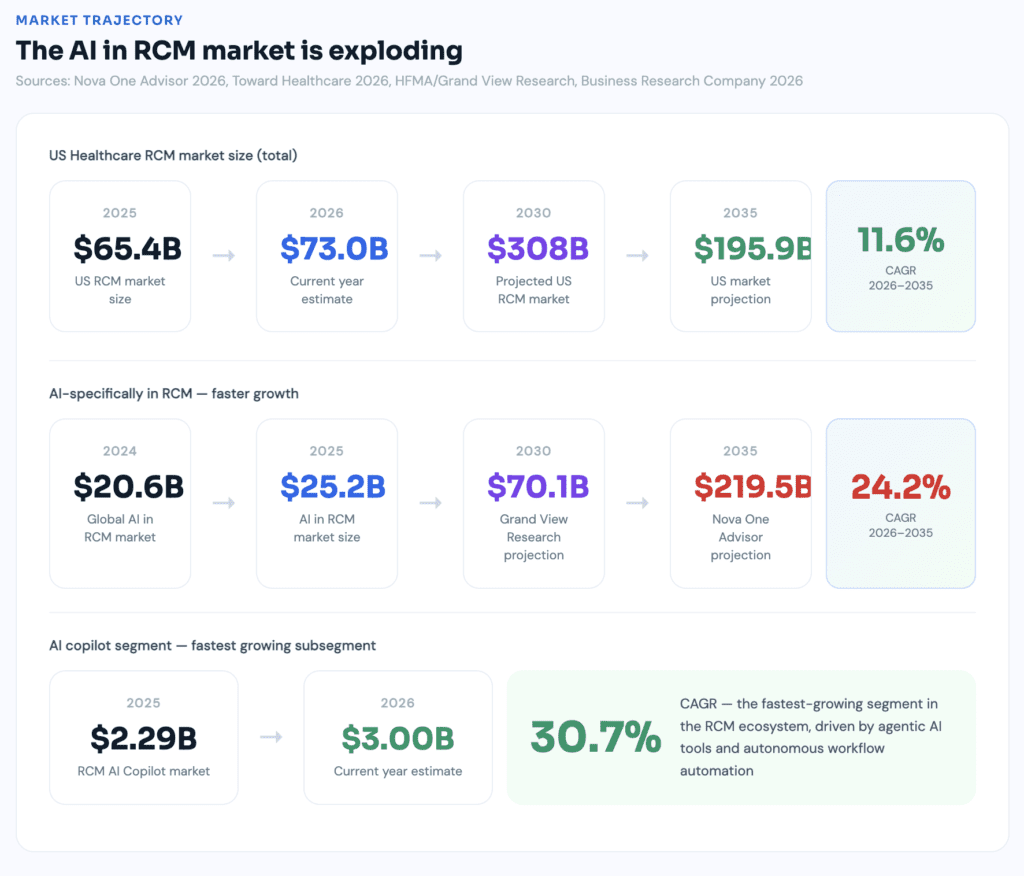
Healthcare denial rates have surged to 11% of all claims, costing providers $19.7 billion annually in denial management expenses alone — and that doesn’t account for delayed revenue, staff burnout, or strategic resources diverted from growth to administrative firefighting. Meanwhile, the U.S. RCM market now totals approximately $90.6 billion and is projected to reach nearly $308 billion by 2030 — a market growing precisely because the problem it serves keeps getting bigger.
Artificial intelligence isn’t a magic wand. But in revenue cycle management, it’s becoming the most consequential operational tool the industry has seen in a generation. The question isn’t whether AI belongs in your billing workflow anymore. That debate is over. The question now is how far behind you’re willing to fall before you act.
What Does “AI in RCM” Actually Mean?
Let’s be precise — because the term gets abused constantly. Every software company slaps “AI-powered” on their dashboard and calls it innovation. So before anything else, let’s define what’s actually happening.
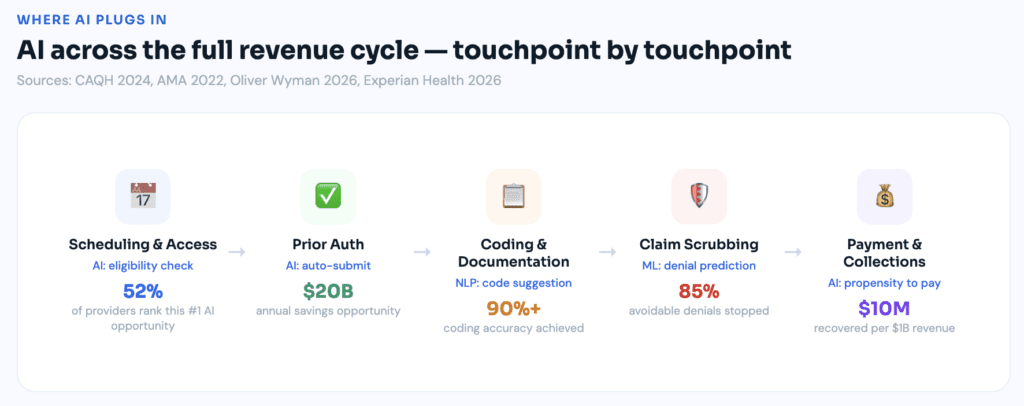
Real AI in revenue cycle management means deploying machine learning, natural language processing, robotic process automation, and predictive analytics across the entire financial and administrative workflow — from patient scheduling all the way through final payment posting. It’s not a single tool. It’s a stack of intelligent systems operating simultaneously across multiple touchpoints.
A machine learning model that scores denial risk before a claim leaves your system. An NLP engine that reads physician notes and suggests ICD-10 and CPT codes with documented rationale. An RPA bot that verifies insurance eligibility overnight without anyone asking it to. A predictive analytics layer that surfaces underpayments your team would never catch manually at scale.
As of 2026, this is no longer theoretical. 63% of healthcare organizations have already integrated AI-powered automation into their revenue cycle workflows, and 80% of health systems report actively exploring, piloting, or implementing generative AI tools for RCM — a 38-percentage-point increase in under two years.
The market is moving. The question for every practice and health system is whether they’re moving with it.
Where Traditional RCM Falls Apart
Here’s something the industry still doesn’t say loudly enough: traditional revenue cycle management was never designed for the environment it currently operates in. It was engineered for a simpler era — fewer payers, simpler code sets, far less compliance overhead. The fragility was baked in from the start.
Clinical documentation happens at the point of care. Coders interpret that documentation — often days later, sometimes with incomplete context. Billers translate codes into claims. Payers process or reject. Every single handoff is a risk point, and the volume of those handoffs has grown dramatically over the past decade.
Experian Health’s 2025 State of Claims data shows that 26% of practices trace at least one in 10 denials back to intake errors: wrong policy numbers, outdated insurance cards, and missed eligibility rechecks. These aren’t complex clinical disputes. They’re administrative failures happening at the front door, before the patient has even sat down.
Then there’s prior authorization. A 2022 AMA survey found that physicians and staff spend an average of nearly 13 hours per week managing prior authorizations — time spent navigating payer-specific portals, compiling clinical documentation, and following up on pending requests for services that, in many cases, could have been flagged and resolved before the appointment was scheduled.
And the financial consequences compound relentlessly. An HFMA Pulse Survey shows hospitals lose an average of 4.8% of net revenue to denials. Meanwhile, HFMA reports that up to 65% of denied claims are never reworked — meaning a significant share of that lost revenue gets written off without a fight. Not appealed. Not corrected. Just gone. One in three hospitals now reports bad debt levels exceeding $10 million — a number that reflects years of accumulated leakage from a system that was never built to catch it.
Key Areas Where AI Is Making a Measurable Difference
1. Stopping Denials Before They Happen
This is where AI delivers its fastest, clearest ROI. Old-school claims scrubbing worked from static rule sets — if a claim has modifier 59 without a supporting diagnosis, flag it. Useful, but it only catches what you already know to look for. It doesn’t learn. It doesn’t adapt. And payer rules change constantly.
AI-powered denial prevention learns from your historical submission data, identifies patterns in what your specific payers reject, and scores incoming claims against those patterns before they ever leave your system. The technology doesn’t just catch today’s errors — it anticipates tomorrow’s.
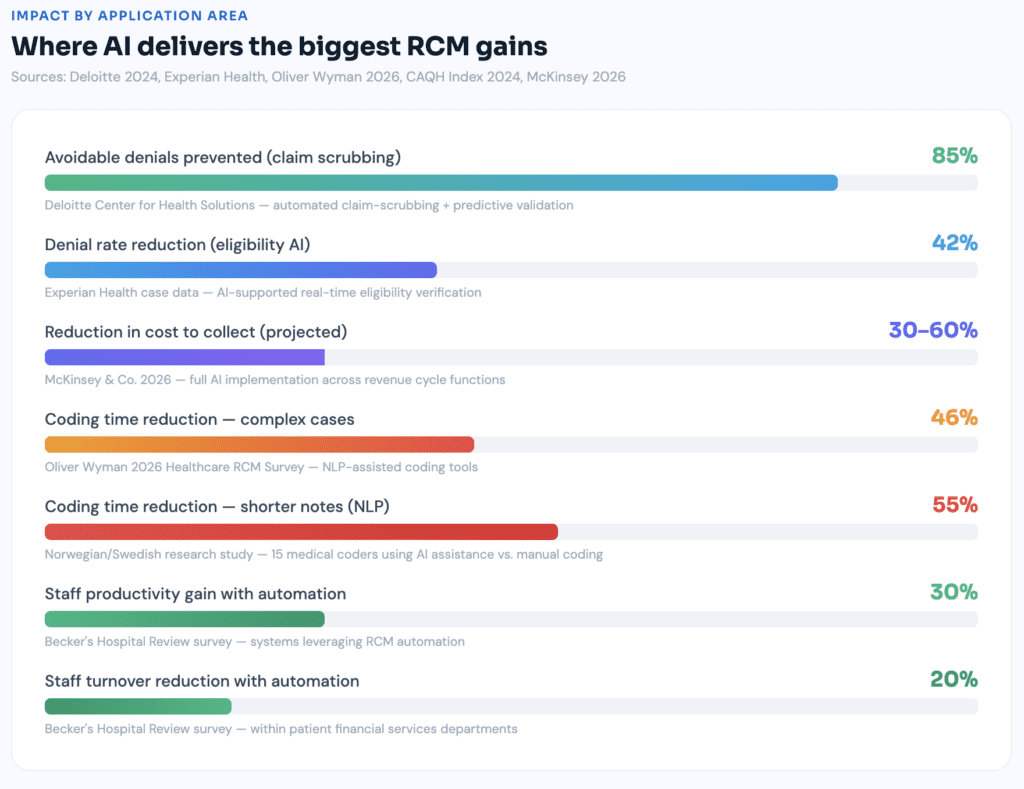
The results are significant. Practices implementing AI-supported eligibility verification have reported cutting denial rates by as much as 42%, according to Experian Health case data. At the system level, Deloitte’s Center for Health Solutions found that automated claim-scrubbing and predictive validation can prevent up to 85% of avoidable denials, reducing administrative cost per claim by nearly one quarter.
That 85% figure deserves a real pause. Most organizations have spent years accepting double-digit denial rates as an unavoidable cost of doing business. It is not unavoidable. It’s a data problem — and AI is designed to solve data problems.
2. Prior Authorization — Finally, Actually Fixed
Prior auth automation might be the single most impactful quality-of-life improvement AI has delivered to billing teams. And I mean that in the most literal operational sense.
The 2024 CAQH Index places the industry-wide savings opportunity from automating eligibility and prior authorization transactions at $20 billion annually. Twenty billion dollars sitting inside manual workflows that technology can largely eliminate. In 2026, investments in automation and AI rank as the biggest RCM priority according to MGMA research, with prior authorization automation leading the list of targeted use cases.
AI-driven PA tools connect directly to EHR systems, extract relevant clinical criteria from documentation, cross-reference payer-specific guidelines, and submit electronically — completing in minutes what once consumed hours per request. More advanced platforms use NLP to read physician notes proactively, identifying which upcoming procedures will require authorization before anyone has to ask.
That shift — from reactive to proactive — changes the entire dynamic. Staff stop chasing approvals and start preventing delays before they happen.
3. NLP-Powered Coding: The Underappreciated Revenue Driver
Coding assistance doesn’t generate as many headlines as denial management, but its financial and compliance impact is significant in both directions — and the stakes are escalating.
The average coding-related claim denial dollar amount rose 126% in 2024 to $631, up from $297. Outpatient coding denials rose a further 26% from 2024 to 2025. Coding errors aren’t a nuisance anymore. They’re a material financial liability with a clear upward trajectory.
NLP tools read raw clinical text — operative notes, discharge summaries, office visit documentation — and suggest codes with supporting rationale pulled directly from the physician’s own documentation. The 2026 data from Oliver Wyman is striking: AI is delivering accuracy rates of 90% or higher in specific clinical coding domains, with studies showing up to 46% reductions in coding time for complex cases.
That productivity gain doesn’t mean coders get eliminated. It means they get leverage. Their expertise gets applied where it actually matters — complex cases, audit response, documentation improvement conversations with clinical staff, and education. The routine gets automated; the judgment stays human.
4. Predictive Patient Payment — Stop Bad Debt Before It Starts
This application surprises people who haven’t encountered it. AI models can now predict, with meaningful accuracy, the likelihood that a specific patient will pay their out-of-pocket balance — and by what method and timeline.
This isn’t about profiling patients. It’s about resource allocation. Collection efforts are finite. If a billing team can route higher-risk patients toward financial assistance programs proactively — before a balance becomes delinquent — both collection rates and patient satisfaction improve simultaneously.
Half of providers say they are “very or extremely concerned” about patients’ ability to pay, up six percentage points from last year. Patient financial risk stratification at the point of scheduling — not at the collections stage — is where this technology creates real, preventive value.
A Real Practice, Real Numbers
An orthopedic group — 12 providers, roughly 4,000 claims monthly — was sitting at a 14% denial rate. High, but not unusual for a specialty combining surgical coding complexity with heavy prior auth requirements from commercial and Medicare Advantage payers.
After implementing an AI-powered RCM platform with denial prediction, NLP coding assistance, and automated authorization workflows, the results over six months were concrete:
- Denial rate dropped from 14% to 6.8%
- Days in A/R fell from 52 to 34 days
- Coder productivity increased 30% — not through cuts, but through volume capacity
- Prior auth turnaround went same-day for 70% of requests, versus 3.2 days before
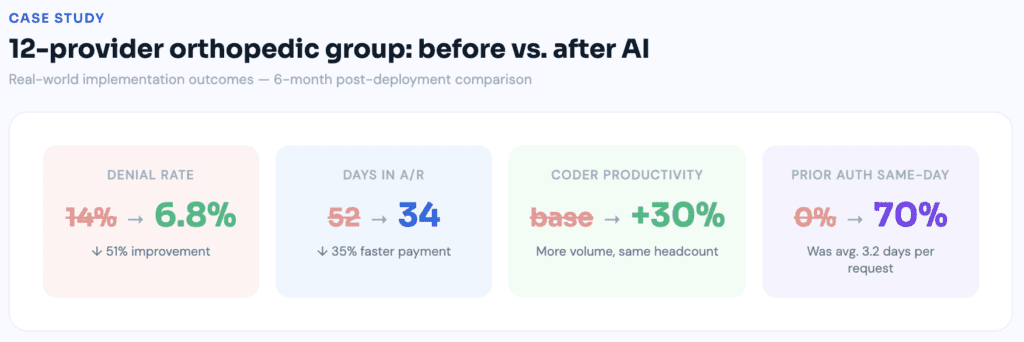
What happened to the billing staff? They were redeployed — from rote data entry into exception management, payer contract analysis, and proactive patient financial counseling. This tracks precisely with what the broader data shows: systems leveraging automation report 30% higher productivity and 20% lower turnover within patient financial services. Less repetitive work means less burnout. Less burnout means lower attrition. Lower attrition means retained institutional knowledge that no platform can replicate.
The Adoption Gap in 2026 — A Shrinking Window
Here’s what should genuinely concern revenue cycle leadership: the window to gain competitive advantage from early AI adoption is closing faster than most organizations realize.
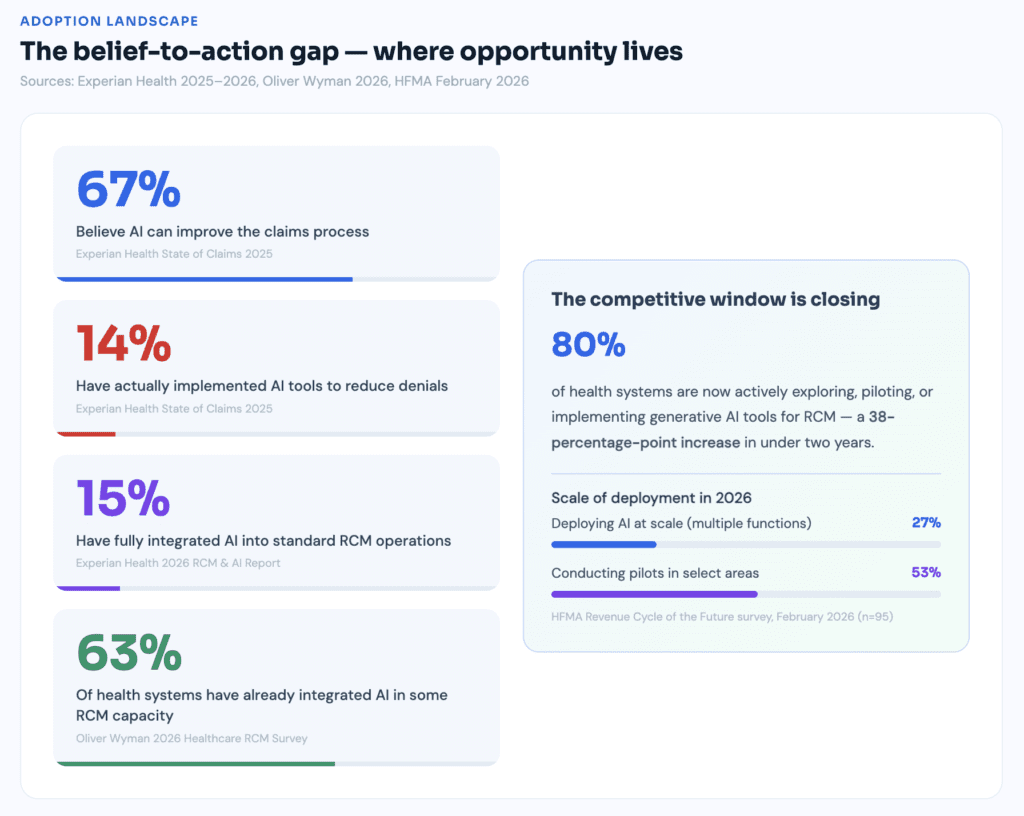
Across the revenue cycle value chain, roughly 20% to 40% of organizations report broad or enterprise-wide use of AI-enabled tools — deployed across a majority of sites and departments rather than confined to isolated pilots. These aren’t experiments anymore. These are production-scale deployments generating compounding performance advantages.
A February 2026 HFMA survey of 95 healthcare finance professionals found that 27% say their organizations are actively deploying AI at scale across multiple functions, and 53% are conducting pilots in select areas. Eighty percent of the industry is either scaling or actively testing. The organizations that are neither are already falling behind.
The payer side isn’t sitting still either. Commercial plan denial rates rose 1.5% while Medicare Advantage plans saw a 4.8% spike from 2023 to 2024. Payers are deploying AI to flag claims that may not meet medical necessity criteria, applying more rigorous scrutiny at a scale no manual review process can match. Telehealth-related denials rose 84% in recent data from MDaudit’s network of 1.2 million providers. The arms race between payer and provider AI systems is already underway. Organizations without AI on the provider side are entering that race unarmed.
The Market Reality — What the Numbers Say About Where This Is Going
The investment data alone tells the story. The AI in RCM market was valued at $25.15 billion in 2025 and is projected to reach $219.48 billion by 2035, growing at a CAGR of 24.19%. That’s not speculative growth — that’s capital following proven ROI at enterprise scale. The revenue cycle AI copilot segment alone grew from $2.29 billion in 2025 to $3.00 billion in 2026, at a CAGR of 30.7%.
On the savings side, AI and automation in the revenue cycle could generate up to $360 billion in annual savings across the industry. McKinsey projects that AI in the revenue cycle could produce a 30% to 60% reduction in cost to collect, faster cash realization, and a workforce refocused on patient value rather than administrative burden.
These aren’t projections made in a vacuum. They’re backed by organizations that have already implemented, measured, and documented the results.
Choosing the Right AI-Powered RCM Solution
Vendor demos are designed to impress. Real evaluations require harder questions.
- Integration depth. Does it connect natively with your EHR, or does data require manual export? 81% of providers now use two or more solutions to collect patient information at check-in, creating inefficiencies that require staff to rerun eligibility checks and manually reconcile data. Adding another disconnected tool compounds that problem.
- Payer-specific training. Has the AI been trained on claims data from your actual payer mix? A model built primarily on Medicare fee-for-service data performs differently against regional commercial payers with unique adjudication rules.
- Transparency in denial logic. Can the system explain why it flagged a claim — not just that it flagged one? Black-box predictions are difficult to act on and impossible to audit.
- Compliance posture. How does the vendor handle PHI? Is the platform HIPAA-compliant with a documented BAA? What are their breach notification policies and data retention timelines?
- Proven results, not projected ones. Request a proof-of-concept using your own historical claims data. Any credible vendor will agree. Hesitation at this ask is a red flag worth taking seriously.
What Vendors Won’t Tell You Before You Sign
AI works better when your underlying data is clean. That sentence seems obvious until you’re three months into an implementation and the model is training on three years of incorrectly coded claims from a previous billing company. Garbage in, garbage out — that axiom doesn’t disappear because machine learning is involved.
The technology is usually the easy part. Just slightly more than half of healthcare finance and revenue cycle leaders describe their teams as “somewhat prepared” or “very prepared” for the revenue cycle of the future, according to HFMA’s February 2026 survey. The gap between system capability and organizational readiness is where most implementations run into trouble — not in the software, but in the people and workflows surrounding it.
AI also doesn’t know your payer contracts. Predictive models can identify patterns suggesting underpayment — but without your contracted fee schedules loaded and actively maintained, the financial recovery opportunity stays theoretical. The Advisory Board estimates that data-driven denial prevention can recover up to $10 million per $1 billion in patient revenue through early intervention and workflow redesign. That recovery is only achievable when contract data management runs alongside the AI tooling.
Expert Tips for a Successful Implementation
- Start with denial prevention, not coding. ROI appears faster, it’s easier to measure, and it builds internal confidence before tackling more complex workflows.
- Audit your data quality before onboarding. Pull 90 days of historical claims and categorize denial reasons by root cause. Fix systematic errors before the AI inherits them.
- Set success metrics before go-live. First-pass acceptance rate. Days in A/R. Cost to collect per claim. Build the reporting infrastructure before anyone touches the new system — otherwise you won’t have a baseline to measure against.
- Involve coders and billers in platform selection. They know where the workflow breaks down. They’ll also be far more invested in a tool they helped evaluate and choose.
- Plan for change management, not just implementation. As one chief revenue officer put it: “It’s the most exciting time to be alive in revenue cycle. But my staff are also feeling that pressure… we’re trying to bring everyone into a modern, more proactive mode. But staff are nervous.” That’s a leadership challenge, not a technology one.
Where This Is All Heading in 2026 and Beyond
Today’s AI in healthcare billing is largely assistive — it flags, suggests, predicts, and alerts. Humans still make most final decisions. The next wave is moving toward genuinely autonomous revenue cycle management.
The market is moving decisively beyond experimentation. Roughly 20% to 40% of organizations now report broad or enterprise-wide AI deployment across the revenue cycle. Agentic AI — systems that don’t just identify problems but take autonomous action to resolve them — is no longer a future concept. It’s entering production at early-adopter health systems right now.
Generative AI is already being piloted for real-time documentation improvement, offering physicians suggestions during note-writing that lock in coding specificity before the encounter closes. Autonomous prior authorization systems are completing submissions end-to-end, with human staff reviewing exceptions rather than processing every request. The direction is unambiguous: fewer human touchpoints on routine transactions, more human expertise applied to genuinely complex decisions.
The outsourced RCM market is projected to nearly double within four years, with 70% of hospitals and health systems planning to expand their RCM outsourcing engagements — a sign that organizations recognize they can’t build every AI capability in-house, and are choosing strategic partnerships to close the gap faster.
Bottom Line
Revenue cycle management has always been a margin game. Collect efficiently, deny less, manage payer relationships proactively — the formula hasn’t changed in decades.
What has changed is the leverage available to execute it. And the cost of not using that leverage is now precisely quantifiable: over 75% of hospital CFOs and revenue cycle leaders identify denials management as their organization’s most time-consuming operational challenge. When senior leadership is consumed by administrative firefighting, strategy suffers. Growth suffers. Patient care suffers.
AI and automation in the revenue cycle could generate up to $360 billion in annual savings across the healthcare industry. That’s not a vendor projection — it’s a measure of how much inefficiency currently exists in a system that was never designed for the complexity it now carries.
The technology exists. The ROI is documented at scale. The 2026 data shows the industry is moving — rapidly — and the organizations that act deliberately now will compound those advantages for years. The ones that wait will find themselves chasing a gap that grows wider every quarter.
Start with a claims audit. Understand where your money is actually going. Then make the case for the technology that stops the bleeding — with numbers your CFO can verify and your payers can’t dispute.
Complete Data Reference Table — 2024, 2025 & 2026
| Statistic | Year | Source |
| Denial rates hit 11.8% | 2024 | HFMA / Kodiak Solutions |
| 41% of providers >10% denial rate | 2025 | Experian Health |
| $19.7B annual denial management cost | 2025 | Experian Health |
| AI cuts denial rates up to 42% | 2025 | Experian Health case data |
| 85% avoidable denials preventable | 2024 | Deloitte Center |
| $20B automation savings (eligibility + PA) | 2024 | CAQH Index |
| 126% rise in coding denial dollar amount | 2024 | MDaudit |
| 65% of denied claims never reworked | 2025 | HFMA |
| Only 14% providers using AI | 2025 | Experian Health |
| 67% believe AI can improve claims | 2025 | Experian Health |
| 30% productivity gain with automation | 2024 | Becker’s Survey |
| 4.8% net revenue lost to denials | 2024 | HFMA Pulse |
| $10M recovery per $1B revenue | 2024 | The Advisory Board |
| 46% coding time reduction (complex cases) | 2026 | Oliver Wyman |
| 90%+ coding accuracy with AI | 2026 | Oliver Wyman |
| 63% of health systems integrated AI in RCM | 2026 | Experian Health / Oliver Wyman |
| 80% of health systems piloting Gen AI for RCM | 2026 | Oliver Wyman |
| 27% deploying AI at scale; 53% in pilots | 2026 | HFMA February 2026 Survey |
| 30–60% reduction in cost to collect (projected) | 2026 | McKinsey |
| U.S. RCM market = $90.6B → $308B by 2030 | 2026 | HFMA / Grand View Research |
| AI in RCM market = $25.15B → $219B by 2035 | 2026 | Nova One Advisor |
| AI + automation = $360B annual savings potential | 2026 | MGMA / Auxis |
| 70% of hospitals expanding RCM outsourcing | 2026 | Auxis |
| 84% rise in telehealth denials | 2025 | MDaudit |
| 1 in 3 hospitals: bad debt exceeds $10M | 2026 | Auxis |
Author Bio

Isaac is a highly accomplished healthcare professional with over 13 years of experience in healthcare administration, medical billing and coding, and compliance. He holds several AAPC specialty certifications and has a bachelor’s degree in Health Administration. He worked previously at a large multi-physician family care and occupational health practice with two locations in northwestern PA and now works for Healthcare Data Central in the ICD-10 Editorial department to write articles about medical billing services. He enjoys sharing his knowledge and experience as a certified PMCC instructor. He has authored many articles for healthcare publications and has been a featured speaker at workshops and coding conferences across the country.



